HDM allergy explained
House dust mite allergy explained
House dust mites (HDMs) are arachnoids and belong to the Pyroglyphidae family. HDMs are present in every household. Living within dust, textile, carpets, beds and upholster furniture (Colloff, 2009). Humans get exposed to HDMs allergens and other indoor allergens on a daily basis. The dust mite itself isn’t harmful to humans and animals, but the real problem is the proteins in their excrements. These proteins are highly allergenic and in response to these allergens humans can become sensitized. A successful development of the house dust mites depends on the presence of food, the temperature and humidity of their habitat. If there is enough food and the circumstances are right the HDMs multiply on a high scale. The female house dust mite can produce around 400 eggs during her lifetime which means that she can produce a new generation of house dust mites every 3 weeks. Even though House dust mites are very small (about 0,1 mm to 1 mm large) and invisible to the naked eye they can cause large problems for humans and animals all over the world.

By Gilles San Martin from Namur, Belgium – House dust mites
House dust mite species
- Dermatophagoides pteronyssinus (European house dust mite)
- Dermatophagoides farinae (American house dust mite)
- Euroglyphus maynei (Mayne’s house dust mite)
The distribution of different sorts of HDMs vary between countries, but also on a global level differences are found (Colloff, 2009). In temperate regions, Dermatophagoides pteronyssinus, Dermatophagoides farinae, and Euroglyphus maynei are the most commonly species found. In tropical and subtropical regions, Blomia tropicalis (family Glycyphagidae) and D. pteronyssinus are the most frequent species, while D. farinae is rarely found in (sub)tropical regions. Studies across the US, Europe, Asia, South America, New Zealand, Australia and Africa have shown that the house dust mites are present globally. Conclusion is that house dust mites can be found almost everywhere in the world but they do not occur at high altitudes (from approx. 1,5 km).
Environment of house dust mites
House dust mites are looking for warm and moisture places. That is why beds are the perfect place for them. HDMs require a temperature between 20-30 degrees Celsius. A relative humidity of around 65-80% and of course the presence of food and molds to feed on. This food can be found in house dust which contains chitin, cellulose and keratin which are derived from human and animal dander. In other words, house dust mites live on the human skin scales and the mold that grows on the human skin scales. All humans loses their skin scales (approx. 1 gram each day) which is enough to feed about 1 million mites. This is the perfect diet for house dust mites.
Sensitization to house dust mites
Humans get exposed to house dust mites allergens and other indoor allergens on a daily basis. The dust mite itself isn’t harmful to humans and animals, but the real trouble makers are the proteins in their excrement’s. These proteins are highly allergenic and in response to these allergens humans can become sensitized. As a result of activities like dusting, bed making, vacuuming or any other activities HDM excitements (with a size of 10-40 µm) and other small allergen carrying particles become temporarily airborne. Free-floating allergens can be inhaled by humans. This happens mainly at night. Humans who are atopic can react on this exposure. Atopic human will make IgE antibodies, which bind to the active immune cells which will stimulate mediators, such as histamine, this can cause a local inflammation. Allergic responses can result in eczema, conjunctivitis, asthma symptoms and rhinitis (Colloff, 2009).
D. pteronyssinus and D. farinae
The majority of house dust mite allergy patients are both sensitized to D. pteronyssinus and D. farinae. The allergens from both of these species are almost always present in house dust samples in temperate areas. Various researchers have described the common allergenic extract components of dust mites. These studies showed that the IgE cross-reactivity between the major allergens Der p 1 and Der f 1 and between Der p 2 and Der f 2 is higher than 80%. Both species contain a significant amount of identical or very similar epitopes that cause immunological cross-reactions.
The life-cycle of house dust mites
House dust mites are poikilothermic and cannot regulate their own body temperature. Therefore their duration of life may vary, depending on the temperature and humidity of their habitat. The life cycle of HDM’s comprise of different stages: egg, 6-legged larva, two phases of 8-legged nymphs, and the final stage is an adult individual. The development from egg to adult, in an optimal laboratory condition, takes 3-4 weeks. The males have a life span of of approx. 70 days. The females live longer, around 100 days. Furthermore the life time depends on the temperature and humidity of their habitat. The female house dust mites make sure that the population will grow, every 3 weeks they produce a new generation of hungry house dust mites. In addition female House dust mites can produce 80 eggs during their life cycle (Colloff, 2009). In their lifetime they produce a large amount of droppings (excrements), the weight of the excrements is around 200 times their own body weight.

Life cycle of house dust mite
The populations fluctuate throughout the season. In general, the size of the populations within the north of Europe are the largest at the end of the summer and autumn. The house dust mite population size declines in the winter. However in autumn, a larger population correlates with increased production of allergens and therefore symptoms of diseases frequently increase in this period. In humid climates the populations are larger in comparison with dry climates (Colloff, 2009).
Why do house dust mites produce allergens?
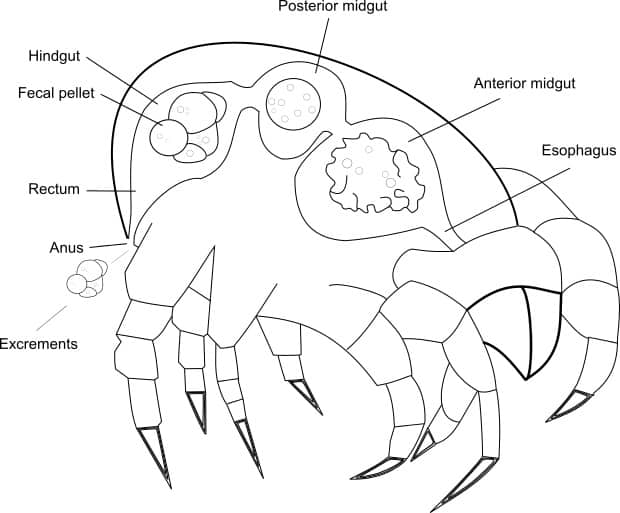
Within HDMs allergens contain a biological functional protein. The paired allergen working is incidental; a bad consequence of the abundant presence of HDM populations within houses. The association of Der p 1 (Group 1 allergens) with the intestinal tract and faecal pellets of HDMs indicate a digestive function. The amino acid sequence of Der p 1 confirms the digestive function (Colloff, 2009). Some other HDM faeces contain other functional enzymes, like amylase. These allergen enzymes were found in faecal pellets extract. Because of this, these enzymes are linked to digestion. Group 2 allergens, like Der p 2, are not present in high concentration in the faecal pellets, therefore they might have another origin (Colloff, 2009).
How do house dust mites produce allergens?
During digestion, cells peel off from the wall of the midgut, together with the swallowed food particles they travel through the intestinal lumen, where food particles are digested. Products of the digestion are absorbed through the intestinal epithelium towards the haemolymph. When cells are at the last part of the intestine, cells are dehydrated and go into apoptose. The faecal pallets are packed in a peritrophic membrane. The peritrophic membrane protects the last part of the intestine for abrasion. The process of digestion results in a high enzyme concentration within the faecal pellets. The faecal pellets have a diameter of approximately 20-50 μm and accumulate within textile where the HDMs live. Proteins are immunogenic (also called allergens) (Colloff, 2009). An allergen is a (non) protein or substance which can induce an allergic response (Galli et al., 2008). Therefore the allergens can trigger an immune reaction when humans are exposed to them. Der p 1 is the first HDM allergen which was discovered and purified, this protein is predominantly present in the faecal pellets. Currently, 23 HDM allergens are known (Colloff, 2009).
Read more about HDM faeces on this page.
Group 1 allergens
Group 1 allergens have a molecular weight of 25 kDa, as monomer, neutral slightly acidic, and polymorph proteins. They belong to the cysteine group of proteolytic enzymes which also contain the mammal enzymes cathepsin B and H, and plant enzymes actinidin and papain. At least 70% of allergic individuals recognize group 1 allergens. These allergens are identified in a lot of HDMs, some of these HDM species are D. pteronyssinus, D. farinae, D. microceras and E. maynei. The allergens can be conceded through the whole body and the faecal pellets. Thereby, allergens get synthesized by cells in the gastrointestinal tract (Colloff, 2009).
Amino acid sequences of group 1 allergens of the pyroglyphids (Dermatophagoides) contains a signal protein of 18/19 residues, followed by a pro-protein of 79/80 residues, the mature protein contains 222-223 amino acids. Other cysteine proteases contain in between transient pre- and pro-forms. The enzyme is produced as inactive and becomes active by cleavage of the pro-protein by autocatalysis (Colloff, 2009).
Mature Der p 1 is a spherical molecule which is folded into two domains, these domains are separated by a surface chasm. The left domain (contains N-terminus and residues: 21-116) is prevailingly an alpha-helix. The right domain (contains C-terminus and residues 117-223) is prevailingly a beta sheet (Colloff, 2009). The final active form of Der p 1 dimerises at a pH of 8, but is a monomer at a pH of 1.5. Authors think that the concentration of Der p 1 within faecal pellets is highly sufficient to exist as a dimer under neutral conditions. Dimerized Der p 1 is more allergenic than the monomeric form. Interestingly, the midgut of the HDM where digestive hydrolysis takes place is slightly acid. Therefore Der p 1 exists as a monomer. In the hindgut were faecal pellets accumulate the environment is neutral to slightly basic. Therefore dimers of Der p 1 are formed in the hind gut. It is known that HDMs have only one Der p 1 gene (Colloff, 2009).
You can find our purified natural Der p 1 here.
Group 2 allergens

Dermatophagoides pteronyssinus (HDM) mite culture
Group 2 allergens are neutral to slightly basic and polymorph. The majority of allergic individuals recognize the 14kDa non-glycosylated allergens. Group 2 allergens are likely to play a role in lipid binding. The exact function remains unknown, it is not likely that group 2 allergens are enzymes. Group 2 allergens are identified in a large number of HDMs compared to other allergens. In D. pteronyssinus, D. farinae, D. siboney, Psoreoptes ovis, Turophagus putrescentiae group 2 allergens are identified (Colloff, 2009).
Complete amino acid sequence of group 2 allergens indicates that allergens get sensitized as pre-proteins with signal proteins of 16-17 residues. Mature protein consists of 125-129 residues. Group 2 allergens are highly conserved. Homolog sequences are not concentrated around the active site and cysteine residues like in group 1 allergens. Group 2 allergens are evenly distributed over the whole molecule. Differences reflect on the phylogenetic relationship of HDM species (Colloff, 2009).
Crystal structure shows a cylindrical molecule that exists of 10 beta strands and a short alpha-helix. It looks like an immunoglobulin like folding which exist of two anti-parallel beta sheets, one exist out of three beta strands, the other of five. The strands overlap each other with an angle of 30° and form a beta-sandwich. Between the different sheets is a central pit where hydrophobic and aromatic residues are lined up. This structure is comparable with other structures found in lipid-binding proteins. Therefore, the structure suggests that group 2 allergens have a lipid-binding function (Colloff, 2009).
You can find our purified natural Der p 2 here.
Diseases associated with HDMs
Over the years, HDMs were regularly linked to different diseases. Most of those diseases have an allergic foundation. The different diseases human suffer from HDMs are, among other things, allergic rhinitis, keratoconjunctivitis, otitis media, allergic asthma, atopic eczema, anaphylaxis, nettle-rash, and gastrointestinal allergy (Colloff, 2009).
Allergic rhinitis
Allergic rhinitis hits 10-30% of the population. The majority (40%) of the population is sensitized to one or more proteins of the environment. In 2012, 9% of all children in the USA were diagnosed with allergic rhinitis the past year. This accounts for 7.5% of the adults within the USA (American Academy of Allergy, Allergy Statistics, 2016). World Health Organization states that 400 million people suffer from allergic rhinitis (WAO, 2011). Most common symptoms of allergic rhinitis are constipated, itchy and or running nose and sneezing (Anafylaxis, 2015). Different investigations show that prevalence rates are increasing over the years, worldwide. Allergic rhinitis is an allergic disease which contains inflammation of the nasal mucosa due to IgE-mediated inflammation. Allergic rhinitis is also a precursor of allergic asthma. Otitis media, sleep disorders, sinusitis, conjunctivitis and sinusitis are some of the co-existing illnesses in line with allergic rhinitis. Controlling the disease includes pharmacotherapy, environmental control measures, patient education and in some cases specific immunotherapy. In Europe the prevalence is approximately 4-32%.
Allergic asthma
Allergic asthma is a life-long chronic inflammatory disorder within the airways. At severe disease structural changes and remodelling of the airway wall takes place (figure 6). Allergic asthma is a common disease among children and adults (Pawankar et al., 2011). Symptoms of asthma include wheezing, shortness of breath, coughing (especially at night), less energy and chest tightness, pain or pressure (Longfonds, 2015). Asthma is associated with airflow obstruction and hyper responsiveness which is most of the time reversible, sometimes medication is needed to reverse the effects. Corticosteroids which need to be inhaled are currently the most effective treatment. The highest identifiable susceptible factor to develop asthma is atopy. Atopy is a genetic marker to develop IgE mediated sensitivity to allergens. Quality of life can get worse for patients with asthma. Asthma is a serious public health problem in the whole world, especially in middle and low income countries. The problem with asthma is that there is no curing therapy yet on the market and there is no worldwide control (Pawankar et al., 2011).
Asthma Statistics, the prevalence of asthma varies globally. Approximately 300 million people have asthma (WAO, 2011). Estimated, 250.000 people die related to asthma each year, these deaths might be unnecessary (American Academy of Allergy, Asthma Statistics, 2016).
HDM allergy affects sleep and quality of life
 One study has shown that allergy symptoms can impair sleep significantly and that the degree of impairment is comparable to the severity of the symptoms. Sleep problems like these can cause fatigue and daytime sleepiness, as well as decreased productivity at work or school, and further lead to impaired learning and memory, depression, and ultimately reduce your quality of life.
One study has shown that allergy symptoms can impair sleep significantly and that the degree of impairment is comparable to the severity of the symptoms. Sleep problems like these can cause fatigue and daytime sleepiness, as well as decreased productivity at work or school, and further lead to impaired learning and memory, depression, and ultimately reduce your quality of life.
The symptoms to look for are:
- blocked or runny nose
- sneezing
- itching and watering eyes
- inflamed eyelids
- shortness of breath
- tight chest
- coughing and wheezing
If you experience some of these symptoms all year round you might be suffering house dust mite allergy and could benefit from consulting your doctor for further clarification. Your doctor can help with diagnosis and the right treatment that can relieve your symptoms.
Diagnosis and treatment of HDM allergy
Your doctor will probably start by asking about the history of your symptoms and conduct a skin prick test that can show if you have house dust mite allergy. Once your doctor knows whether you are allergic to house dust mites and has determined the severity of your symptoms, the next step will be to select the most suitable treatment for you.
“In deciding the best treatment for someone who suffers from house dust mite allergy, the intention is to provide a treatment that will reduce the symptoms, including allowing the person to sleep better at night and function better during the day as a result of feeling fully rested again. Furthermore, house dust mite allergy is closely linked to the development of asthma, emphasizing the importance of treating the condition,” says Jørgen Nedergaard Larsen.
HDM allergen concentrations exposure linked to sensitization
There is some, but not consistent, evidence that levels of exposure are linked to the risk to get sensitized by HDMs within childhood. This is not valid for other types of allergens. The levels of exposure associated with sensitization may vary geographically. Exposure to HDM allergens varies enormously around the world. Where HDM allergen levels are high, atopic sensitization will be more abundantly present. The prevalence of asthma and atopic sensitization are in general not consistently linked to dust HDM exposure in infants and children. Research, where only allergen prevention was used to prevent children from developing asthma, gave disappointing results. Levels of allergen exposure are associated with asthma within atopic adults who are sensitized to HDMs (Colloff, 2009).
Population densities of HDMs
The spread and quantity of HDMs is dependent on their favourable microclimate where they can live and reproduce. HDM population densities influence allergen levels, human exposure and, with a certain reach, prevention of severity of disease. Microclimates indoor are influenced, at least for a certain part in the year, due to the outside climate, also within good isolated houses. The influences of macroclimate on HDM populations appear, on regional and global scales, to overwrite the indoor microclimate. Still, some HDM species do not differ around the world. The most common HDMs and their allergens like D. pteronyssinus and D. farinae are common globally. In houses were the outdoor climate is beneficial for the largest part of the year (like moist and high temperatures) all houses contain HDMs (Colloff, 2009). Humidity is an important factor for the prevalence of HDMs, inside and outside the house. High concentrations of HDMs are found within damped houses. The most favourite place to stay of the HDMs is the bed; warmth, moisture and nourishment. The bed is relative humid and this increases rapidly when an individual goes to sleep (Calderon et al., 2015).
Easy HDM control methods
Some HDM control methods which could help the reduction of allergens:
- Impermeable mattress covers
- Ventilate mattress daily
- Change sheets at least once a week and wash at high temperature
- Reduce the humidity in the bed by leaving the sheet folded back from the mattress
- Daily airing of the room, reduce the humidity by opening windows and doors
- Keep the room temperature under 20 degrees
- Tea tree-oil can be added to (minimalizes bacterial growth) when cold wash,
- Remove carpet and curtains from bedroom
- Frequently dust with a damp cloth
- Vacuum weekly all carpets and upholstered furniture with a HEPA filter, or use a steam cleaner.
- When living in a climate where the summer is hot and sunny and the winters cold and dry: put outside upholstered furniture, mattresses, sheets, carpets and textile for 12 hours, after this vacuum-clean (Colloff, 2009).
Possible treatments
There are many options for treating your house dust mite allergy. The options range from over-the-counter (OTC) and prescription symptomatic medicines, to more long-term treatments like allergy immunotherapy. The two overall ways of treatment have both shown to provide relief and put an end to the discomfort and the sensation of feeling ill, but there are some differences:
Symptomatic treatments work while taking the medicine, but have no long-term effect. They reduce the symptoms of allergy, but unlike allergy immunotherapy, do not induce tolerance. Most symptomatic treatments are available over-the-counter (OTC), e.g. in supermarkets or pharmacies. Symptomatic treatments can include antihistamines, nasal and inhaled steroids and decongestants.
Allergy immunotherapy treatment has a long-term effect with sustained improvement, including in the years following treatment. The main difference between symptomatic and immunotherapy treatment is that immunotherapy induces tolerance and alters the natural course of the disease.
Choosing a treatment option that is right for you should be decided in close consultation with your doctor. Influencing factors include the cause of your allergy and how severe your symptoms are.
We provide pharmaceutical source material for the production of HDM immunotherapy, these include mite bodies and whole cultures.
Why are HDMs still a problem?
It is difficult to control HDMs and their allergens. Many methods, mentioned above, seem not effective and do not work to reduce the allergen exposure (Colloff, 2009). A review of P. C. Gøtzsche et al. (2008), covered 54 trials which included control measures to reduce the exposure to HDMs and their allergens. Looking at the 54 trials there was no beneficial effect demonstrated by using any of the used control measures. The numbers of the control group and number of the patients who had less symptoms after the investigation where similar. The asthma symptom scores and medication usage where similar for both the control and the treated group. There was no difference measured in severity of asthma between both groups. Therefore, physical and chemical methods are both found to be ineffective (Gøtzsche et al., 2008).
F.M.D. Fu-Sheng Wu et al (2012). investigated daily vacuuming of mattresses, thereby decreasing numbers of HDM allergens, β-glucan and endotoxin. Daily vacuuming of mattresses has shown to reduce exposure to bio-contaminants. Combining vacuuming with other methods, like encasing the mattress, it probably will reduce the exposure to allergens even more. The problem of vacuum mattresses is that non-sensitized human need to do the vacuuming. Due to airborne particles, sensitized human are not able to enter the room for at least half an hour after cleaning (Fu-Sheng Wu et al., 2012).
Regarding a meta-analysis of W.D. Arroyave et al. (2014), impermeable HDM covers did not primary prevent allergic diseases and or tertiary prevent respiratory symptoms of diagnosed allergic patients. Although nasal symptoms scored slightly better in the tertiary prevention experiments, it was not significant. The trend in nasal symptoms was not sufficient when lower-quality studies were removed. Even if the quantity of HDMs in mattresses was decreased significantly, there was no evidence that health improved in atopic human. To conclude, impermeable HDM covers are not effective in reducing symptoms or preventing the development of allergic diseases (Arroyave et al., 2014).
The determination of reduction of allergen exposure remains difficult, a reduction might work for one patient, but may be too frail for another. Another problem is that HDMs are everywhere, and every human carries them (Colloff, 2009). HDMs and humans are indissolubly linked due to the fact that HDMs feed on human skin. The human skin indirectly influences the habitat of the HDMs (Calderon et al., 2015). The positive side is that more methods are developed to measure personal allergen exposure. There is an increase in knowledge of behaviour and dynamic processes of allergens indoor (Colloff, 2009).